Prophylactic cerebrospinal fluid drainage and spinal cord ischemia in thoracic and thoracoabdominal endovascular procedures: a systematic review and meta-analysis
Abstract
Background: Spinal cord ischemia (SCI) is one of the most devastating complications of thoracic endovascular aortic repair (TEVAR). Prophylactic cerebrospinal fluid drainage (CSFD) has been shown to decrease the risk of SCI in open thoracic aortic procedures; however, its utility in TEVAR remains uncertain. This systematic review and meta-analysis aim to determine the role of prophylactic CSFD in preventing SCI in TEVAR.
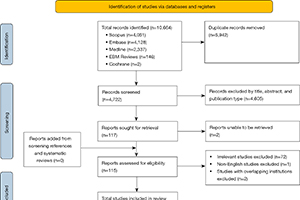
Methods: A literature search of five databases was performed and all studies published before September 2022 that reported SCI rates in TEVAR patients undergoing prophylactic CSFD were included. A random effects meta-analysis of means or proportions was performed for single-arm data. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported for comparisons between groups.
Results: A total of 4,793 patients undergoing TEVAR from 40 studies were included. The mean age was
68.8 years and 70.9% of patients were male. The overall SCI rate was 3.5%, with a 1.3% rate of immediate SCI and a 1.9% rate of delayed SCI. There were no significant differences in SCI rates between prophylactic CSFD patients and non-drained patients. Routine CSFD did not have a significant impact on SCI rates compared to non-drained patients. There was an increased rate of transient SCI with selective CSFD compared to non-drained patients (OR 2.08; 95% CI: 1.06–4.08; P=0.03). The most common drain-related complication was spinal headache (4.3%). The major complication rate was 1.6%, of which epidural or spinal hematoma (0.9%) was the most common, followed by intracranial or subdural hemorrhage (0.8%) and paraparesis or paraplegia (0.8%).
Conclusions: This study found no significant difference in SCI rates between prophylactic CSFD patients and their non-drained counterparts. CSFD is associated with a small but non-negligible risk of serious complications. Multi-center randomized controlled trials (RCTs) are warranted to help stratify the risk of both SCI and CSFD-related complications in patients undergoing endovascular aortic procedures.
Cover