Pulmonary endarterectomy in severe chronic thromboembolic pulmonary hypertension: the Toronto experience
Abstract
Background: Pulmonary endarterectomy (PEA) in severe chronic thromboembolic pulmonary hypertension (CTEPH) is associated with higher risks. However, recent evidence suggests that these risks may be mitigated with the use of extracorporeal membrane oxygenation (ECMO).
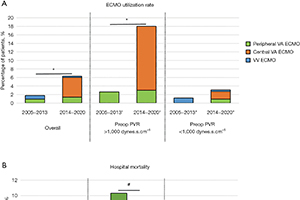
Methods: We performed a retrospective analysis of 401 consecutive patients undergoing PEA at the Toronto General Hospital between August 2005 and March 2020. Patients with severe CTEPH defined by pulmonary vascular resistance (PVR) >1,000 dynes.s.cm–5 at the time of diagnosis were compared to those with PVR <1,000 dynes.s.cm–5Results: The New York Heart Association (NYHA) functional class, brain natriuretic peptide (BNP) and 6-minute walk distance were worse in patients with PVR >1,000 dynes.s.cm–5. A greater proportion of patients with PVR >1,000 dynes.s.cm–5 was treated with targeted pulmonary hypertension (PH) medical therapy (38% vs. 18%, P<0.001) and initiated on inotropic support (7% vs. 0.3%, P<0.001) before PEA. Since 2014, the ECMO utilization rate increased in patients with PVR >1,000 dynes.s.cm–5 compared to those with PVR <1,000 dynes.s.cm–5 (18% vs. 3.1%, P<0.001). The hospital mortality in patients with PVR >1,000 dynes.s.cm–5 decreased from 10.3% in 2005–2013 to 1.6% in 2014–2020 (P=0.05), while the hospital mortality in patients with PVR <1,000 dynes.s.cm–5 remained stable (1.2% in 2005–2013 vs. 2.7% in 2014–2020, P=0.4). The overall survival reached 84% at 10 years in patients with PVR >1,000 dynes.s.cm–5 compared to 78% in patients with PVR <1,000 dynes.s.cm–5 (P=0.7).
Conclusions: The early and long-term results of PEA in patients with severe CTEPH are excellent despite greater postoperative risks. ECMO as a bridge to recovery after PEA can be useful in patients with severe CTEPH.
Cover