Total arch replacement using selective antegrade cerebral perfusion as the neuroprotection strategy
Abstract
Background: Optimal neuro-protection strategy in aortic arch surgery is a controversial issue. The present study reported surgical outcomes of total arch replacement using selective antegrade cerebral perfusion (SACP).
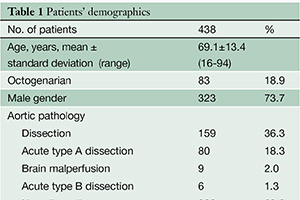
Methods: From January 2002 to December 2012, 438 consecutive patients (mean age 69.1±13.4 years) underwent total arch replacement using SACP through a median sternotomy. Acute aortic dissection was present in 86 patients (18.3; 80 type A, 6 type B) and shaggy aorta in 36 (8.2%). Emergent/urgent surgery was required in 144 (32.9%). Our current approach included: (I) meticulous selection of arterial cannulation site and type of arterial cannula; (II) selective antegrade cerebral perfusion; (III) maintenance of minimal tympanic temperature between 20 and 23 ℃; (IV) early re-warming after distal anastomosis; and (V) maintaining fluid balance below 1,000 mL during cardiopulmonary bypass. A woven Dacron four branch graft was used in all patients.
Results: Overall hospital mortality was 4.6% (20/438). Hospital mortality was 9.7% (14/144) in urgent/emergent surgery and 2.0% (6/294) in elective cases. Permanent neurological deficit occurred in 5.3% (23/438) of patients. Prolonged ventilation was necessary in 58 patients (13.2%). Multivariate analysis demonstrated that risk factors for hospital mortality were octogenarian (OR 4.45, P=0.03), brain malperfusion (OR 23.52, P=0.002) and cardiopulmonary bypass time (OR 1.07, P=0.04). The follow-up was completed in 97.9% with mean follow up of 2.3±2.3 years. Survival at 5 and 10 years after surgery was 79.6±3.3% and 71.2±5.0% respectively. In the acute type A dissection group, 10-year survival was 96.8±2.9%, while in the elective non-dissection group 5- and 10-year survival were 81.4±7.2% and 77.0±5.9% respectively.
Conclusions: Our current approach for total aortic arch replacement utilizing SACP was associated with low hospital mortality and morbidities leading to favorable long-term outcome.
Cover