Aortic valve replacement using stented or sutureless/rapid deployment prosthesis via either full-sternotomy or a minimally invasive approach: a network meta-analysis
Abstract
Background: New technologies such as sutureless or rapid deployment prosthetic valves and access via minimally invasive incisions offer alternatives to traditional full-sternotomy aortic valve replacement (SAVR). However, a comprehensive comparison of these surgical techniques along with alternative valve prosthesis has not been completed.
Methods: Electronic databases were searched for studies comparing outcomes for SAVR, minimally invasive AVR (MiAVR), sutureless/rapid-deployment AVR (SuAVR) via full-sternotomy, or minimally invasive SuAVR (MiSuAVR) from their inception until September 2018. Early postoperative outcomes and follow-up data were included in a Bayesian network meta-analysis.
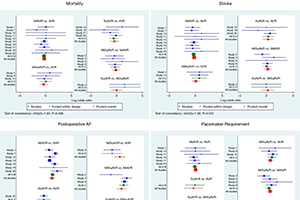
Results: Twenty-three studies with 8,718 patients were identified. Compared with standard SAVR, SuAVR had significantly lower incidence of postoperative AF [odds ratio (OR) 0.33, 95% confidence interval (CI): 0.14–0.79, P=0.013] and MiSuAVR greater requirement for postoperative permanent pacemaker (OR 2.27, 95% CI: 1.25–4.14, P=0.008). All sutureless/rapid-deployment procedures had reduced cardiopulmonary bypass and cross-clamp times, by a mean of 25.9 and 25.0 min, respectively. Hospital length of stay (LOS), but not intensive care LOS, was reduced for all groups (MiAVR −1.53 days, MiSuAVR −2.79 days, and SuAVR 3.37 days). A signal towards reduced early mortality, wound infections, and acute kidney injury was noted in both sutureless/rapid-deployment and minimally invasive techniques but did not achieve significance. Sutureless/rapid-deployment procedures had favourable survival and freedom from valve related reoperation, however follow-up times were short and demonstrated significant heterogeneity between intervention groups.
Conclusions: Minimally invasive and sutureless techniques demonstrate equivalent early postoperative outcomes to SAVR and may reduce ventilation time, hospital LOS and postoperative atrial fibrillation (POAF) burden.
Cover