Alcohol septal ablation: in which patients and why?
Abstract
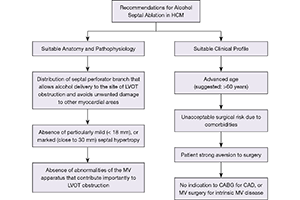
At present, surgical septal myectomy is regarded as the “gold standard” treatment for most patients with obstructive hypertrophic cardiomyopathy (HCM) and drug-refractory symptoms. However, the best results are obtained by those surgeons who have extensive experience with this operation at a small number of referral centers. In the mid-1990s, percutaneous alcohol septal ablation was introduced as an alternative to myectomy to reduce LV outflow gradient and heart failure symptoms in patients with obstructive HCM. However, certain features of alcohol ablation limit its applicability to carefully selected patients. Because this procedure involves the injection of 1–4 mL of 96% ethanol into a septal perforator of the left anterior coronary artery to produce a myocardial infarction (with septal thinning, outflow tract widening and gradient reduction), alcohol ablation is limited by the size and distribution of the septal perforator branches. In addition, rich blood supply from other septal branches not occluded by the balloon and from the posterior descending coronary artery may restrict myocardial ischemia to portions of the septum that do not contribute to outflow obstruction. Septal hypertrophy may be either mild or particularly marked, and abnormalities of mitral valve apparatus may also play a major role in outflow obstruction. When such features are present, alcohol-induced septal thinning is unlikely to significantly reduce the gradient. In addition, persisting uncertainties regarding the risk for ventricular tachyarrhythmias after alcohol ablation suggest this procedure should be limited to patients of advanced age, patients at unacceptable operative risk due to comorbidities, or those with strong aversion to surgery. Further progress in the treatment for patients with obstructive HCM and severe refractory symptoms will come from assuring proper patient selection for alcohol septal ablation, as well as increasing the number of surgeons and centers experienced in performing septal myectomy.
Cover