Salvage esophagectomy for persistent or recurrent disease after definitive chemoradiation
Abstract
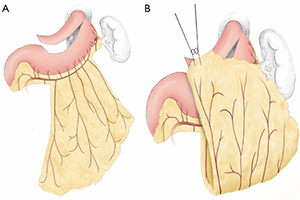
Locoregionally advanced esophageal cancer is treated by some oncologists with definitive chemoradiation. The optimal strategy to treat persistent or recurrent disease after definitive chemoradiation is controversial. We reviewed the literature to determine current treatment options and optimal approaches. Salvage esophagectomy of relapsed or recurrent esophageal cancer has traditionally been associated with increased risk. Modern literature, however, suggests that in specialized high volume centers the risk of salvage esophagectomy when accompanied with various risk-reducing approaches (anastomosis in non-radiated esophagus, omental transposition, selective use of alternative conduits and two stage procedures) is similar to planned esophagectomy after neoadjuvant chemoradiation. Long-term survival rates following salvage esophagectomy are also achievable and similar to planned esophagectomy. Since there are no other potentially curable treatment options, we recommend that all physiologically fit patients with locoregionally persistent or recurrent esophageal cancer after definitive chemoradiation be referred to a specialized high volume esophageal center for salvage esophagectomy.
Cover