Is the outcome in acute aortic dissection type A influenced by of femoral versus central cannulation?
Abstract
Background: The purpose of this study was to evaluate the single-center experience in initial femoral versus central cannulation of the extracorporeal circulation for acute aortic dissection type A (AADA).<
Methods: Between January 2003 and December 2015, 235 patients underwent repair of AADA. All patients were evaluated for the type of arterial cannulation (femoral vs. central) for initial bypass. Demographic data and outcome parameters were accessed.
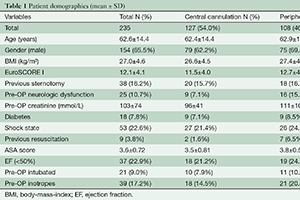
Results: One hundred and twenty seven (54.0%) were initially cannulated in the central aortic vessels (ascending aorta or subclavian/axillary artery) and 108 (46.0%) in the femoral artery. Patients were comparable between age (62.4±14.4 vs. 62.9±14.4 years, P=0.805), gender (male, 62.2 vs. 69.4%, P=0.152) and previous sternotomy (15.7 vs. 16.7%, P=0.861) between both cannulation groups; while EuroSCORE I (11.5±4.0 vs. 12.7±4.2, P=0.031) and ASA Score (3.5±0.81 vs. 3.8±0.57, P=0.011) were significantly higher in the femoral artery cannulation group. Bypass (249±102 vs. 240±81 min, P=0.474), X-clamp (166±85 vs. 157±67 min, P=0.418) and circulatory arrest time (51.6±28.7 vs. 48.3±21.7 min, P=0.365) were similar between the groups as were lowest temperature (18.1±2.0 vs. 18.1±2.2, P=0.775). Postoperative neurologic deficit and 30-day mortality were comparable between both cannulation groups (11.7 vs. 7.2%, P=0.449 and 20.2 vs. 16.9%, P=0.699, central vs. peripheral cannulation). Multivariate analysis revealed only EuroScore I above 13 as single preoperative predictor for mortality.
Conclusions: AADA can be operated with both femoral and central cannulation with similar results. Risk for early mortality was driven by the preoperative clinical and hemodynamic status before operation rather than the cannulation technique.
Cover