Comparison between antegrade and retrograde cerebral perfusion or profound hypothermia as brain protection strategies during repair of type A aortic dissection
Abstract
Background: The goal of this study was to compare early postoperative outcomes and actuarial-free survival between patients who underwent repair of acute type A aortic dissection by the method of cerebral perfusion used.
Methods: A total of 324 patients from five academic medical centers underwent repair of acute type A aortic dissection between January 2000 and December 2010. Of those, antegrade cerebral perfusion (ACP) was used for 84 patients, retrograde cerebral perfusion (RCP) was used for 55 patients, and deep hypothermic circulatory arrest (DHCA) was used for 184 patients during repair. Major morbidity, operative mortality, and 5-year actuarial survival were compared between groups. Multivariate logistic regression was used to determine predictors of operative mortality and Cox Regression hazard ratios were calculated to determine the predictors of long term mortality.
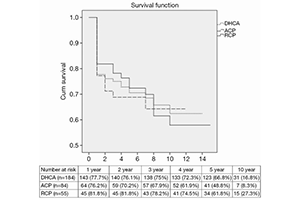
Results: Operative mortality was not influenced by the type of cerebral protection (19% for ACP, 14.5% for RCP and 19.1% for DHCA, P=0.729). In multivariable logistic regression analysis, hemodynamic instability [odds ratio (OR) =19.6, 95% confidence intervals (CI), 0.102–0.414, P<0.001] and CPB time >200 min(OR =4.7, 95% CI, 1.962–1.072, P=0.029) emerged as independent predictors of operative mortality. Actuarial 5-year survival was unchanged by cerebral protection modality (48.8% for ACP, 61.8% for RCP and 66.8% for no cerebral protection, log-rank P=0.844).
Conclusions: During surgical repair of type A aortic dissection, ACP, RCP or DHCA are safe strategies for cerebral protection in selected patients with type A aortic dissection.
Cover